Introduction
Active engagement with music is known to affect myriad brain structures, cortical circuits, and mental/cognitive functions, including emotion and memory, with the associated benefit of stimulating neuroplasticity.1 By contrast, regions/systems of the brain mediating these processes—particularly the amygdala, hippocampus, anterior cingulate cortex, corpus callosum, and hypothalamic-pituitary-adrenal axis—are associated with structural and functional alterations following experienced trauma,2,3 particularly childhood maltreatment, including abuse/neglect, and other adverse childhood experiences. In 2022, researchers at the Upadhyay lab at Boston Children’s Hospital proposed a biobehavioral framework correlating maltreatment experienced during vulnerable stages of child development with neurobiological changes that may precipitate aberrant processing of pain and contribute to the development of psychiatric illness. They theorized that a complex interplay of maladaptive and protective factors contributes to phenotypic outcomes in the aftermath of trauma experienced during childhood.4
Although the neuroscience of music’s adaptive influence—and trauma’s deleterious influence—on brain development has been extensively studied, clinical research is limited regarding what effects live music participation might have on trauma-reactive symptomatology in the specific setting of a long-term psychiatric residential treatment facility (PRTF) for children.5,6 In their scoping review of music therapy research published on youth with adverse childhood experiences, Abrahams and colleagues further underscore the need for methodologically rigorous, well-designed studies to strengthen conclusions about the effects of music-based intervention among this population.6
With these considerations in mind, we designed a retrospective single-arm cohort study examining what effects live music therapy (LMT) had on mitigating trauma reactivity among 12 patients at an inpatient PRTF for youth ages 8 to 12 years who experienced childhood maltreatment (Table 1). Additional PRTF program acceptance criteria included previous hospitalization for harm to self or others and failure of less restrictive environments. Building from the aforementioned conceptual model, a central premise of our study is the hypothesis that sustained, active engagement with live music, by promoting neuroplasticity and positively modulating attention/arousal, can serve as a significant protective mechanism countering the maladaptive neurobiological changes associated with childhood maltreatment. Accordingly, we hypothesize that regular participation in LMT, understood as an inherently active and interactive form of music therapy, can help reduce externalizing behaviors and, by extension, involvement in psychiatric emergencies (codes) as well as receipt of as-needed medications (PRNs) among youth hospitalized at trauma-focused PRTFs.
Methods
To test our hypotheses, we conducted chart review of unit documentation regarding primary outcome measure of change in externalizing symptoms, as well as secondary outcome measure of change in internalizing symptoms (eg, depression, anxiety, social withdrawal), among the study population before, during, and after participation in once-weekly, hour-long LMT sessions (the intervention). LMT took place over an 8-week period as an option for patients during regularly scheduled recreational therapy time, which included alternatives such as coloring/drawing, gameplay, or other leisure activities. Participation was voluntary, and the study was reviewed/approved by an institutional review board. The concept grew from a child and adolescent psychiatry fellowship training experience, in which the first author (M.L.) volunteered to play/teach guitar and sing popular songs with patients every Friday for 8 weeks during a clinical rotation at the PRTF.
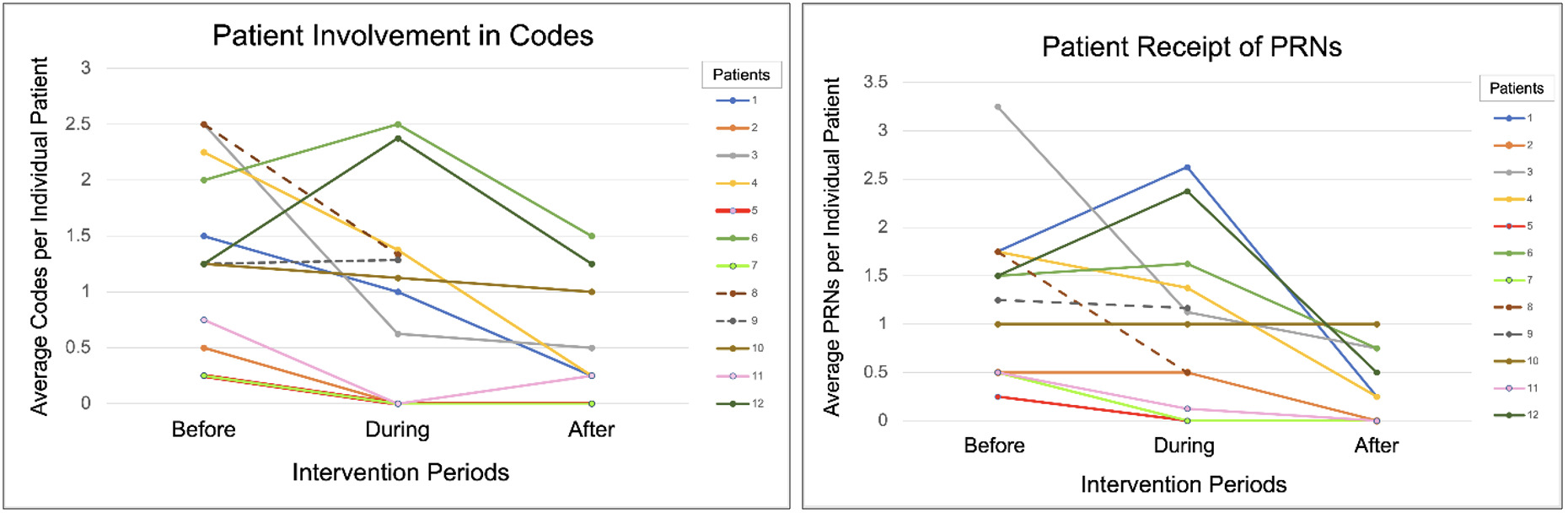
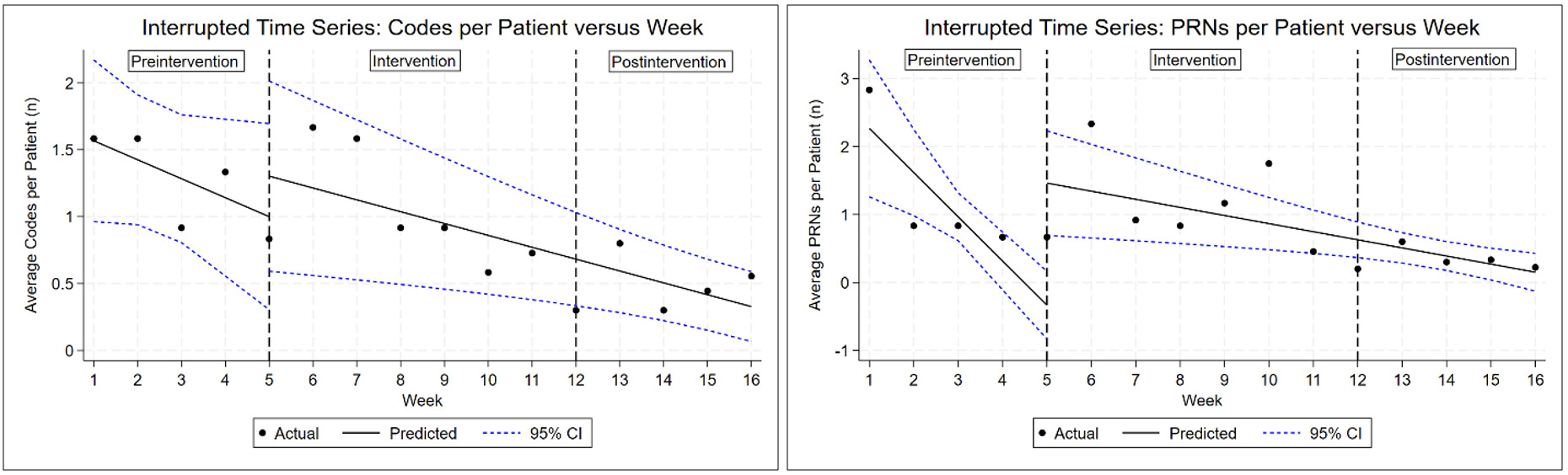
Change in externalizing symptoms (eg, behavioral dysregulation, verbal/physical aggression) was measured by documentation of patient involvement in codes and number of PRNs received due to agitated behavior, while change in internalizing symptoms was measured by patient self-report of mood, for the 4 weeks before, 8 weeks during, and 4 weeks after the intervention. These time frames were maximized to the extent possible, with limitation by the unpredictable nature of admissions/discharges on the unit. Average codes and PRNs were initially calculated for each patient per intervention period, followed by interrupted time series (ITS) analysis looking at change in collective average codes and PRNs per week. ITS was chosen to assess available longitudinal data in context of a preintervention/postintervention structure but no true control group due to logistic constraints.
Results
Following 8 weeks of LMT, roughly 90% of patients showed a downtrend in average codes and PRNs (Figure 1). Change in internalizing symptoms was less prominent with roughly 50% of patients reporting a generally euthymic mood during the same period. While objective data pertinent to change in externalizing symptoms were readily available/quantifiable, retrospective analysis made change in internalizing symptoms harder to standardize/quantify and limited this outcome measure to mood self-report; use of prospectively selected, validated assessment tools would help address this in a future iteration of such a study.
_by_individual_patient_(intervent.png)
Although ITS analysis reflected a net reduction in average codes and PRNs during and following the intervention (Figure 2), it is not possible to say from this whether LMT was contributory beyond treatment as usual (TAU). Of note, the rate of decrease in average weekly codes was not statistically significant before LMT began but became statistically significant after the intervention; however, the model’s estimate of the intervention’s contribution to this rate of change was positive and not statistically significant by itself. Likewise, the rate of change to average daily PRNs was sharply negative before LMT began and became less sharply negative afterward, while the model’s estimated impact of the intervention was positive.
_analysis_on_unit_average_codes_and_receipt_of_as-needed_medi.png)
Discussion
Our ITS findings seem to have been driven in part by an idiosyncratically high number of PRNs administered during weeks 1 and 6. Thus, these effects may have been driven by specific patients in specific weeks. All these findings must be interpreted with caution in light of the small study population and lack of a true comparator group. While our intention had been to analyze outcomes against a control of similar patients for whom the intervention had not been offered, practical limitations led us to choose ITS analysis as a means of creating a preintervention/postintervention comparison. A larger, preferably multicenter, study comparing LMT implementation to a cohort of similar patients engaged with another music-based intervention (such as receptive listening to recorded music rather than active participation in LMT), other modes of arts-based therapy (such as painting and/or creative writing), and/or TAU alone, would be necessary to determine whether engagement with LMT contributed to the outcome measures beyond TAU.
In an ideal world, TAU in a trauma-focused long-term PRTF for youth occurs in a therapeutic milieu where medication management, psychotherapy, and schooling take place over a period of 4 to 6 months. In such a treatment setting, it is to be expected that TAU would lead to a progressive reduction in trauma-reactive symptomatology, which was observed in our study. Our hypothesis that LMT would steepen the downward slope in codes and PRNs, however, was not observed. Numerous factors may have impacted patient response to LMT, including but not limited to unit milieu, school/psychosocial stressors, peer/staff reactivity, psychiatric medication adjustments, trauma-informed therapy response, individual music taste, and duration/frequency of the intervention.
Variability in length of stay complicates continuity of cohort participation in such a study, accounting for the shorter pre-LMT/post-LMT periods (4 weeks) vs the intervention period (8 weeks), which we recognize as a limitation. The small sample size in this single-site pilot study (N = 12), while consistent with typical inpatient units for trauma-reactive youth given the unique behavioral challenges such patients demonstrate, also reduces the power of our findings. However, it is precisely within this population/setting that we would anticipate a more robust response to LMT in terms of potential for externalizing symptom mitigation.
Conclusion
This retrospective single-arm cohort study aimed to investigate the effects of LMT at a trauma-focused inpatient PRTF for children. To our knowledge, this is the first published attempt to assess the objective outcome measures of change in codes and PRNs after music-based intervention in such a setting. While we were unable to separate the effects of LMT from TAU due to the lack of a control group, our results support further study. As outcome measures did continue to improve after the addition of LMT, we suggest that it would be an interesting progression of this project to design a prospective multiarm cohort study with a comparator group and standardized intervention model, ideally including increased duration/frequency of LMT sessions led by trained facilitators with music selection tailored to match patient interests. Our hope is that this pilot study may serve as a foundation for future research investigating the role LMT could play in attenuating acute externalizing symptomatology among trauma-reactive youth hospitalized at PRTFs with a potential benefit of reducing overmedication among this at-risk population.
Plain Language Summary
Hospitalized youth who have experienced trauma often present with externalizing symptoms, including physical aggression, which can lead to psychiatric emergencies (codes) and administration of as-needed medications for behavioral stabilization.
This pilot study examined whether regular engagement with live music therapy made a difference in reducing trauma-reactive symptomatology and, by extension, involvement in codes as well as receipt of as-needed medications among 12 patients at an inpatient psychiatric residential treatment facility for youth ages 8 to 12 years who experienced childhood maltreatment.
Following 8 weeks of live music therapy, roughly 90% of patients showed a downtrend in average codes and as-needed medications. Although we were unable to separate the effects of live music therapy from treatment as usual due to study limitations, our results support further investigation of the role live music therapy could play in attenuating acute externalizing symptomatology in trauma-reactive youth at psychiatric residential treatment facilities with a potential benefit of reducing overmedication among this at-risk population.
About the Authors
Mats Lemberger, MD, is a Child and Adolescent Psychiatrist at the Geisel School of Medicine at Dartmouth, DHMC Department of Psychiatry, Lebanon, New Hampshire, USA.
Chuchitra Thanigaivasan, MD, is a Resident in the Department of Pediatrics, Authority Health, Detroit, Michigan, USA.
Stephen Holley, MD, is a Resident in the Department of Psychiatry, LewisGale Medical Center, Salem, Virginia, USA.
Ron Carico Jr, PharmD, MPH, is a Clinical Pharmacist at the Joan C. Edwards School of Medicine at Marshall University, Department of Psychiatry, Marshall Health Network, Huntington, West Virginia, USA.
Stephanie Gao, MD, is an Assistant Professor of psychiatry at the Joan C. Edwards School of Medicine at Marshall University, Department of Psychiatry, Marshall Health Network, Huntington, West Virginia, USA.
Robert Sears, MD, is an Assistant Professor of psychiatry at the Joan C. Edwards School of Medicine at Marshall University, Department of Psychiatry, Marshall Health Network, Huntington, West Virginia, USA.
Correspondence to:
Mats Lemberger, MD; email: mathew.s.lemberger@hitchcock.org, 603-650-7075.
Funding
The authors have reported no funding for this work.
Disclosure
The authors have reported no biomedical financial interests or potential conflicts of interest.
Acknowledgments
We wish to thank Dr Laura Adkins and Dr Darshana Shah for their guidance as well as the Marshall Department of Psychiatry and River Park Hospital in Huntington, West Virginia, for supporting our research.