Introduction
Children’s mental health (MH) in the United States has been and currently remains in crisis. Primary care settings have been increasing the integration of MH services through increased access and multidisciplinary partnering, but financial compensation remains a significant barrier to fostering integrative care. Certain policies and environments do not incentivize sustained funding for integrated care approaches. Regardless, 2 integrated care models have proven efficient in collaborating with MH providers.
Integrated Care Delivery Models
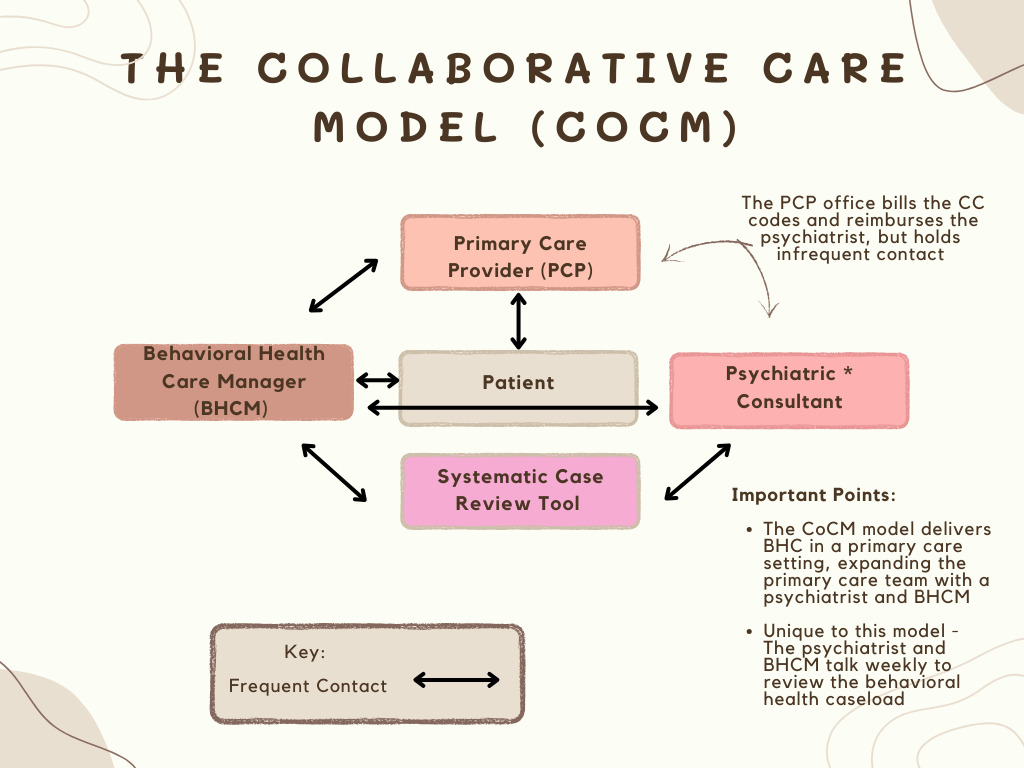
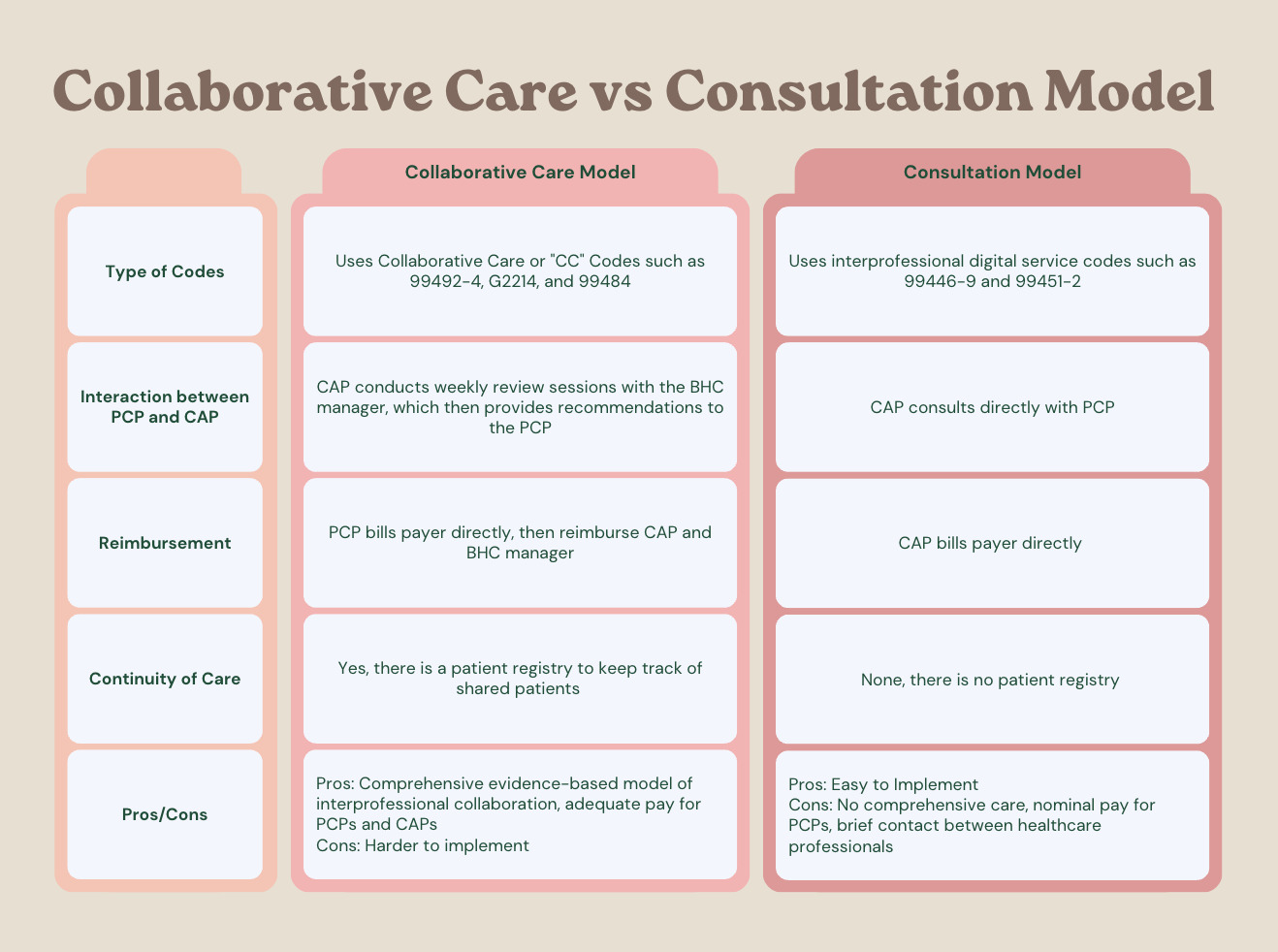
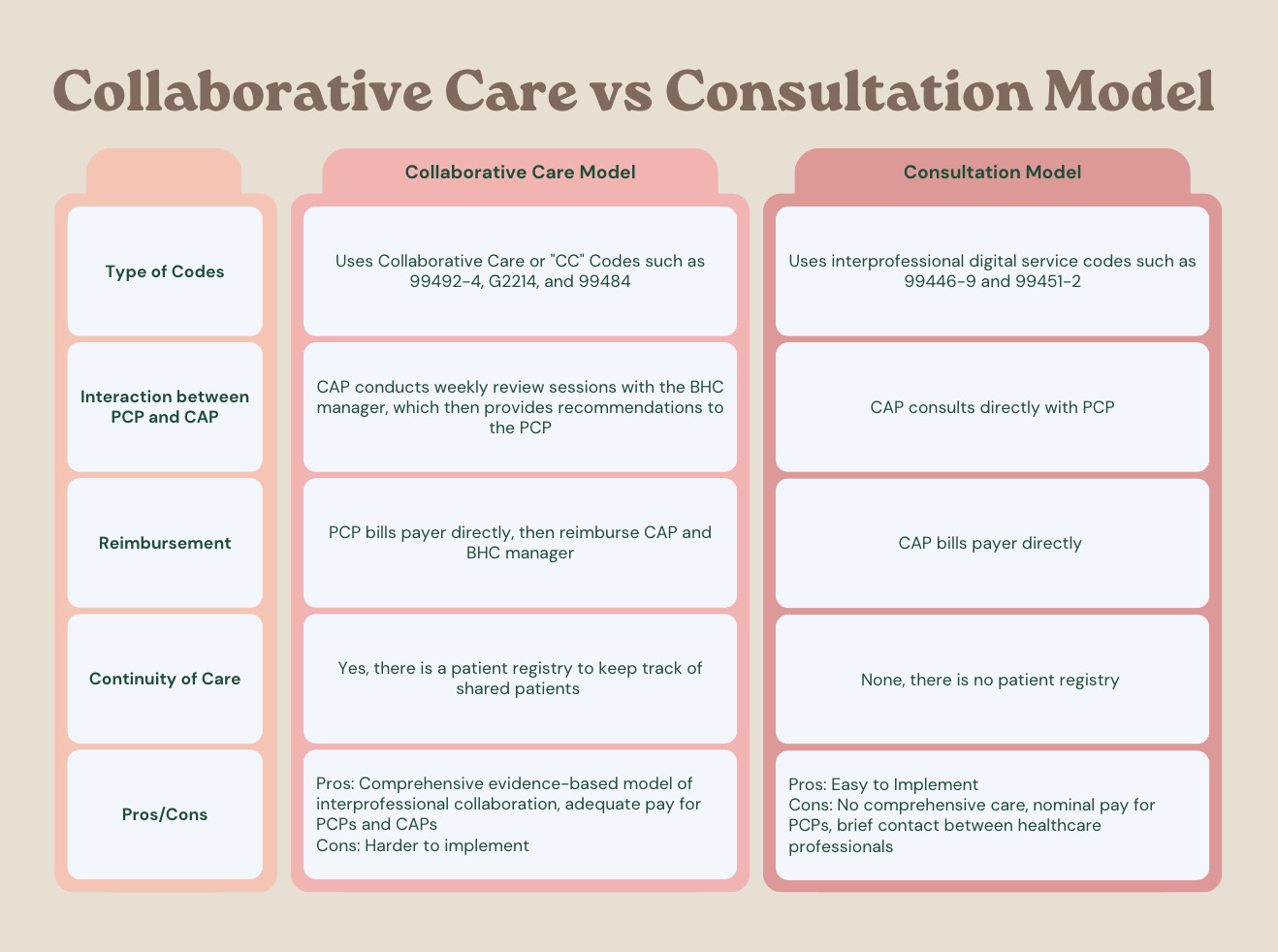
The first model is the comprehensive collaborative care model (Figure 1), which uses “collaborative care” (CC) codes and emphasizes the use of screening tools to identify patients in need of services. Under the Washington Collaborative Care Model (AIMS CoCM), psychiatrists work with the Behavioral Health Care Manager (BHCM), review the registry of patients, and make recommendations that are shared with the primary care provider (PCP). Essentially, BHCM has specialized training in behavioral health (social work, nursing, or psychology), working under the oversight and direction of the billing PCP.1 BHCM follows up proactively between the PCP and the child and adolescent psychiatrist (CAP) while providing care management services, which include conducting brief psychosocial interventions and maintaining the patient registry. Patients are entered into a registry, which is a database or caseload management tool that tracks patients’ engagement and symptom improvement.1 The CAP serves as a consultant who supports the PCP and the BHCM in treating children with MH problems in concert with their parents or caregivers. Typically, the CAP conducts weekly review sessions with the BHCM. Ideally, a CAP would directly evaluate the patient when needed, while providing recommendations to the PCP or BHCM via phone or in person, within varied allotted times. However, this is atypical and varies within different integrated systems that follow the AIMS CoCM model.
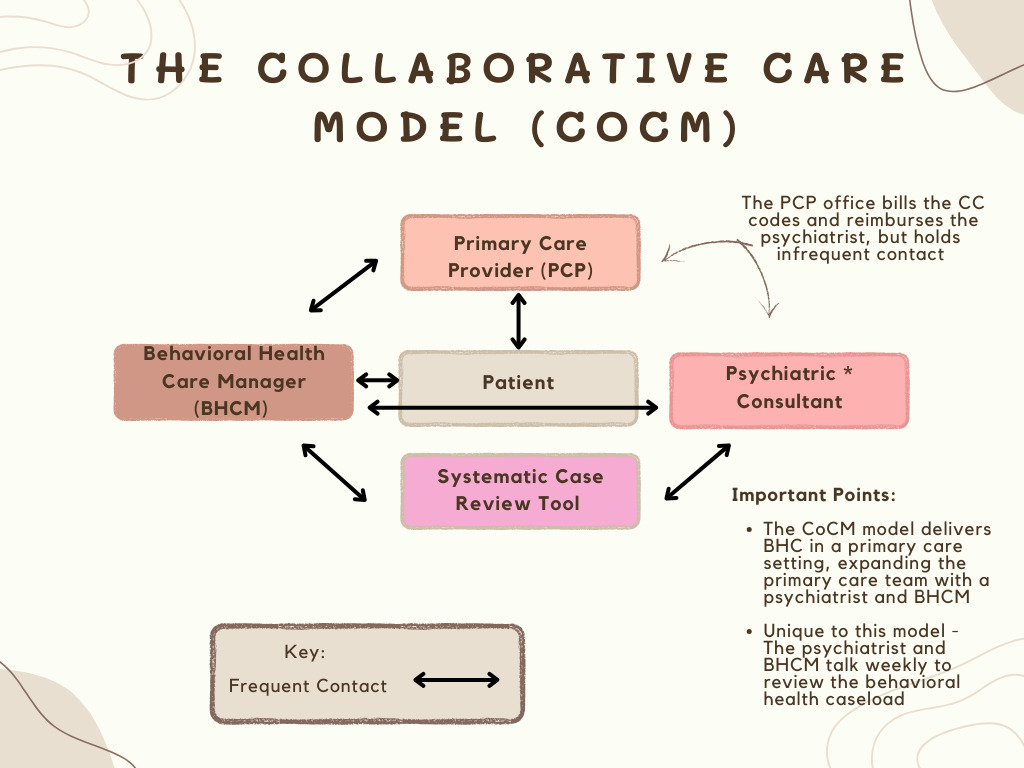
In general, CC codes from the CC model exhibit a more comprehensive evidence-based model of interprofessional collaboration. Because everything is logged into the registry, specific screening tools and outcome measurements such as the Patient Health Questionnaire (PHQ-9) can be utilized to determine if patients’ conditions are improving. PCP invoices the payer monthly using a per-patient, per-month CPT billing code. The time is based on all the BHCM services, including a patient’s time reviewing with the psychiatrist. The code is weighted so that there is an inherent payment for the psychiatrist’s time built in, which can be paid either hourly or via salary to the psychiatrist and BHCM, and contains money for the PCP and the primary care practice overhead and workflow. The more patients in the registry, the higher the collection each month. Any time spent by the BHCM can be potentially billed by the PCP on a per-patient, per-month basis using CC codes. CC provides opportunities for collaboration, not only with primary care teams, but also with fellow MH clinicians, community organizations, and schools. In support of this model, Burkhart et al conducted a systematic review of integrated and CoCMs in pediatric primary care and found that these models are associated with increased MH treatment initiation and completion, higher patient satisfaction, and improved child adaptive behavior and MH outcomes.2
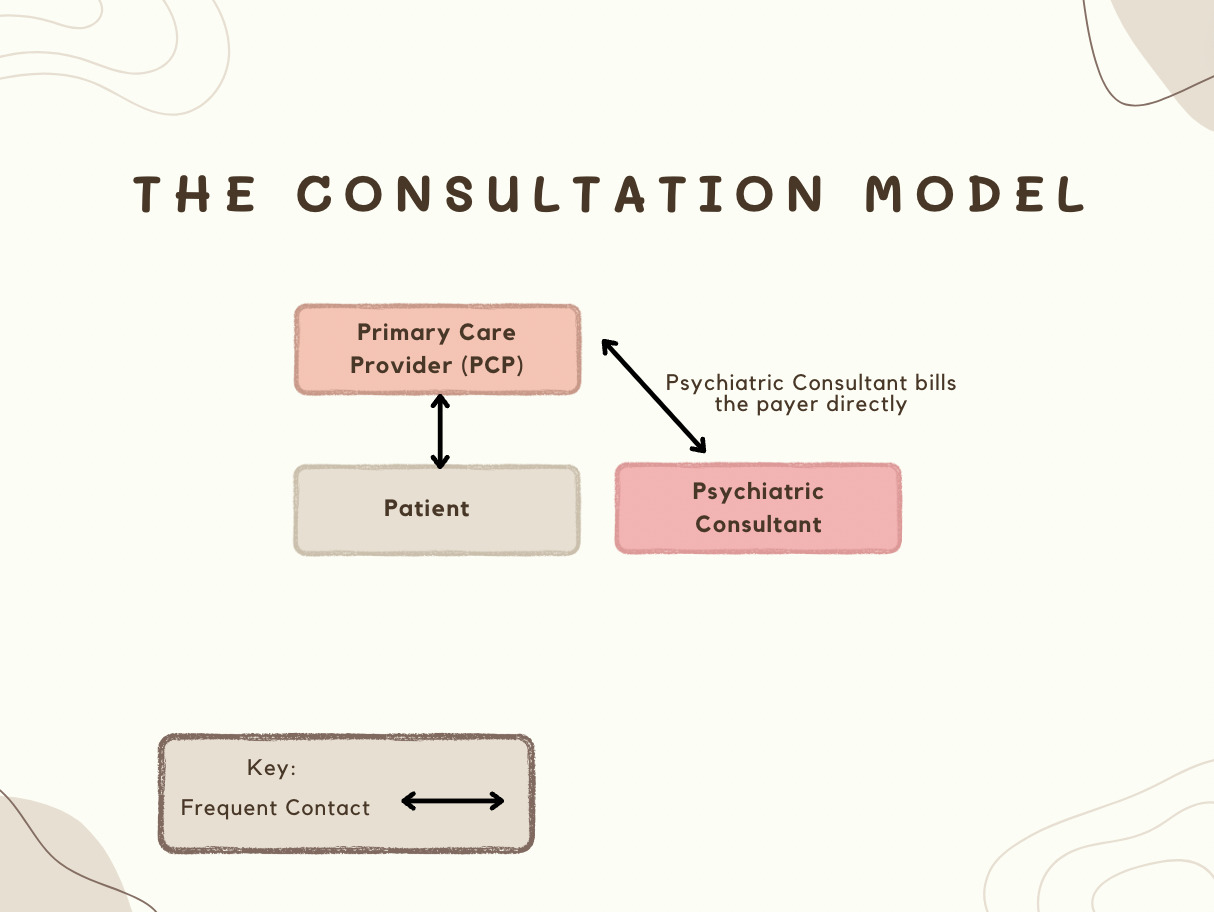
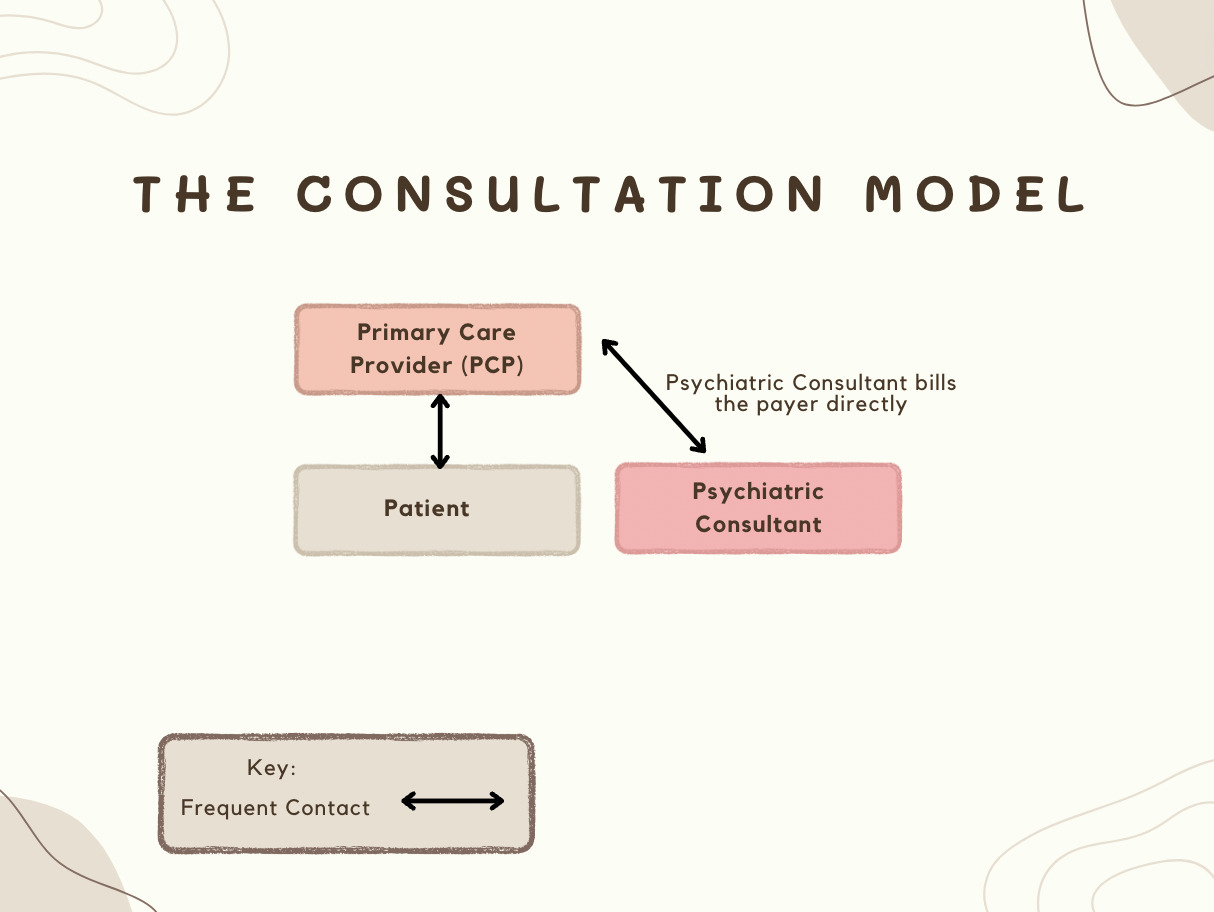
The second model is a flexible consultation model (Figure 2) where the PCP consults directly with a CAP and the CAP bills the payer directly for professional-to-professional services on behalf of the patients using interprofessional digital service codes (Figure 3). Since CAPs bill directly, they are not dependent on billing or reimbursement through PCPs. However, the consultation codes require patient information to be collected for the CAP to bill the insurance directly. Inadvertently, this creates the view of a doctor-patient relationship and may result in potential liability. There is also no continuity of care for CAPs, no registry, and no measures to track if the patients are clinically improving, so it is not as comprehensive as the CoCM model. However, an advantage of the consultation model is that it works well for brief contacts between professionals, without the patient present, and is easy to implement.
Integrated Care Payment Models
Insurance Reimbursement
Ideally, all states should say “yes” to the CoCM model if there is compensation at a reasonable rate. Recently, North Carolina and New Jersey received statewide approval for Medicaid reimbursement of CC codes, requiring 120% of the Medicare fee schedule for reimbursement. This means PCPs are paid even if patients are seen in school or at a clinic. This is a significant step for CC in terms of expanding accessibility and improving patient stabilization, as it allows patients to address their MH concerns without having to miss school or work. Increasingly commercial insurers, state Medicaid programs, and Medicaid managed care carve-outs are covering CC codes, securing additional funding for many states and making CoCM a sustainable model for many primary care practices.
Currently, it is difficult to compare the revenue of both CC and interprofessional digital service codes. However, sustainable funding of these codes should be through their seed funding, which includes both grants and commercial insurers. Medicaid reimburses through CC codes, bundled payments, and capitated payments such as value-based payment programs (VBPs). VBPs reward providers based on the quality of their services rather than the traditional fee-for-service payment models, which is advantageous for patients and their families. However, there are many barriers to implementing VBPs as a reimbursement strategy due to the state variations in Medicaid reimbursement and the fact that cost savings for children take longer to accumulate than for adults. As a result, this does not incentivize payers and health care organizations to invest in programs that take years to impact outcomes and costs.3 Additionally, barriers to linking data, sharing data, and pooling funding make it difficult to assess children’s comprehensive health and social needs.4 Limited data exists on pediatric VBPs, and few examples are available to guide pediatricians in implementing alternative payment models with appropriate metrics. Despite limited data and challenges in implementation, pediatric VBPs still hold promise for long-term benefits in improving both the accessibility and quality of behavioral health care.
Federal Block Grant Funding to States
The approval of the Consolidations Appropriation Act includes 3 bills, including the CC bill, which sets aside grants for behavioral health integration. The CC bill essentially funnels money to the Substance Abuse and Mental Health Services Administration (SAMHSA), which subsequently issues block grants to the states.5 Each state sets up a granting program that provides seed funding for small practices. With this new funding from the SAMHSA grants, states and small practices now have additional financial help to jumpstart a CoCM model.
Program Grants
An example of a specialized consultation model is the Health Resources and Services Administration (HRSA) funded “child psychiatry access programs” (CPAP) or “pediatric mental health care access programs,” where CAPs provide informal MH consultation to PCPs regarding medications or psychiatric diagnoses via evidence-based brief interventions or telepsychiatry across all 50 states.6,7 The federal government, or individual states, can fund CPAPs via grants or a consortium of payers to provide the technical assistance needed to adopt pediatric integrated care.
State Assessments
States also use a mixture of assessments on insurers to finance CPAPs, with the most common approaches being per-member-per-month (PMPM) fees and premium-based percentage assessments. PMPM fees are a fixed-dollar amount charged for individuals enrolled in a health plan within a given month. Premium-based percentage assessments involve charging insurers a percentage of the gross premiums they earn from health plans sold in the state. For example, Pennsylvania and Massachusetts CPAPs use an insurer-supported PMPM framework in which MCO entities or commercial carriers make contract-required PMPM payments to cover a defined share of CPAPs’ operating costs.8
Since PCPs collaboratively assess and manage MH concerns of children within both the CoCM and consultation model, this promises potential cost savings. As supported by the Milliman report, the effective integration of medical and behavioral care can potentially save $26–48 billion annually in general health care costs, and most of the projected reduced spending is associated with facility and emergency room expenditures in hospital facilities.9 Children and caregivers both benefit from decreased psychiatric emergency department visits and inpatient psychiatric hospitalizations. Integrated care brings upon earlier intervention, more time to discuss prevention, fewer missed school days for children, and consequently fewer missed workdays for parents. As PCPs care for more patients under an integrated model, it paves the way for expanding services. Referral rates to CAPs within the same hospital network increase, which generates additional revenue. Although CAPs are in no shortage of patients and referrals, CAPs are ethically improving outcomes by helping as many children as possible in collaboration with pediatricians.
Overall, these 2 types of integrated care models improve access to MH in patients’ local zip codes and reduce the financial burden of MH services. Dissemination and fiscal sustainability are barriers to such models. However, with increased education, advocacy, and the noted need for integrated care services, insurers are slowly overcoming these barriers. Hence, these models act as primary interventions and have great potential to alleviate the current children’s MH crisis.
Plain Language Summary
Integrated care models can alleviate the current crisis for children’s mental health (MH). We aim to describe how these models can increase MH access, while advocating for their financial sustainability. We found that these models can contribute to potential cost savings within a collaborative system. However, the billing codes for these models need to pay well to incentivize physicians to participate. Fortunately, increasingly commercial insurers, new bills, and state Medicaid programs are covering these financial costs. Once long-term financial sustainability is ensured, these models have the opportunity to comprehensively manage psychosocial problems and aid providers in enhancing their clinical practice.
Author contributions
Writing – review & editing: Sammi Wong (Lead), Mark Borer (Supporting). Supervision: Xiao Xiong You (Supporting).
About the Authors
Sammi Wong, DO, Resident Physician, OBH Brookdale University Hospital Medical Center, 1 Brookdale Plaza, Brooklyn, New York, USA.
Xiao Xiong You, MD, Attending Physician, OBH Brookdale University Hospital Medical Center, 1 Brookdale Plaza, Brooklyn, New York, USA.
Mark Borer, MD, DLFAPA, DLFAACAP, Owner, Psychiatric Access for Central Delaware, P.A 846 Walker Rd. Ste 32-2 Dover, Delaware, USA.
Correspondence to:
Sammi Wong, DO; email: sawong@bhmcny.org, (718) 240-5667.
Funding
This project did not receive any funding.
Disclosure
Dr. Wong reports no biomedical financial interests or potential conflicts of interest. Dr. You reports no biomedical financial interests or potential conflicts of interest. Dr. Borer reports that he is a paid consultant to the quality improvement committee of Highmark DE Health Insurance. The NAMI Delaware Advisory is funded by HRSA grant for Delaware Child Psychiatry Access Program (DCPAP). Dr. Borer is a paid consultant for CoCM Program with Delaware Pediatrics and is the former chair of the Delaware Medicaid Pharmacy and Therapeutics Committee and Drug Utilization Review Boards.
This study was presented at the AACAP 2024 Meeting; October 14–19, 2024; Seattle, Washington.