
Introduction
In 2022, suicide remained the second leading cause of death for adolescents aged 10–14 years and the third leading cause of death for those aged 15–19 years.1 There has been a corresponding rise in studies examining the characteristics and precipitating circumstances of youth both attempting and dying by suicide.2,3 However, there are surprisingly limited data examining youth who survived medically serious suicide attempts (MSSAs), even though evidence suggests they are at higher risk for eventually dying by suicide.4 This study examined youth admitted to a pediatric hospital for medical treatment following a suicide attempt to explore associated demographics, psychosocial contributors, and clinical histories, as well as different age trends over time. The goal was an improved understanding of factors associated with youth suicide attempts involving subsequent medical instability to inform more effective prevention and treatment strategies.
Methods
This retrospective chart review obtained data from youth aged 10–17 years who were admitted to our 65-bed pediatric tertiary hospital in northern New England, from January 2016 to December 2021, following a known suicide attempt. Age limit was determined by the hospital admission criteria. Two forms of electronic chart queries were performed. Epic analysts completed a search using relevant keywords for admission. Charts were additionally identified using the Epic Slicer Dicer tool.
Charts were excluded for incidents of accidental injury, including recreational substance use. Study data were limited to the first medical admission for a suicide attempt to make inferences specifically about initial admissions and avoid patient duplication.
Data points collected are reflected in Table 1. Age at admission was dichotomized into 2 groups to reflect national data groupings: ages 10–14 and 15–17. We used the American Psychological Association’s definition of a “psychosocial crisis,” specifically a situation producing significant cognitive or emotional distress. Group differences were determined by Fisher’s exact tests. We used χ2 tests for simple descriptive bivariate analyses, including N, percentages, and P values (Table 1). For associations related to the study’s aims, we ran linear regression models and included the test statistic with associated confidence intervals and P values. Additionally, Table 1 includes adjusted P values reflecting the application of a False discovery rate. This study was deemed exempt from full IRB review by the MaineHealth IRB and was conducted in accordance with all relevant ethical guidelines.
Results
Data from 188 eligible patients were included for analysis. Patients were almost equally split between age groups. Analyses by natal sex and gender revealed no clear differences between age groups. However, there was a notable difference between age groups in both male (20% vs 40%, P = .012) and female gender (75% vs 60%, P = .012). Natal sex followed a similar trend. Only a small portion of the patient population identified as transgender. Rurality had no meaningful association (see Table 1, Demographics). Any chronic medical comorbidity was <1% and not listed in Table 1.
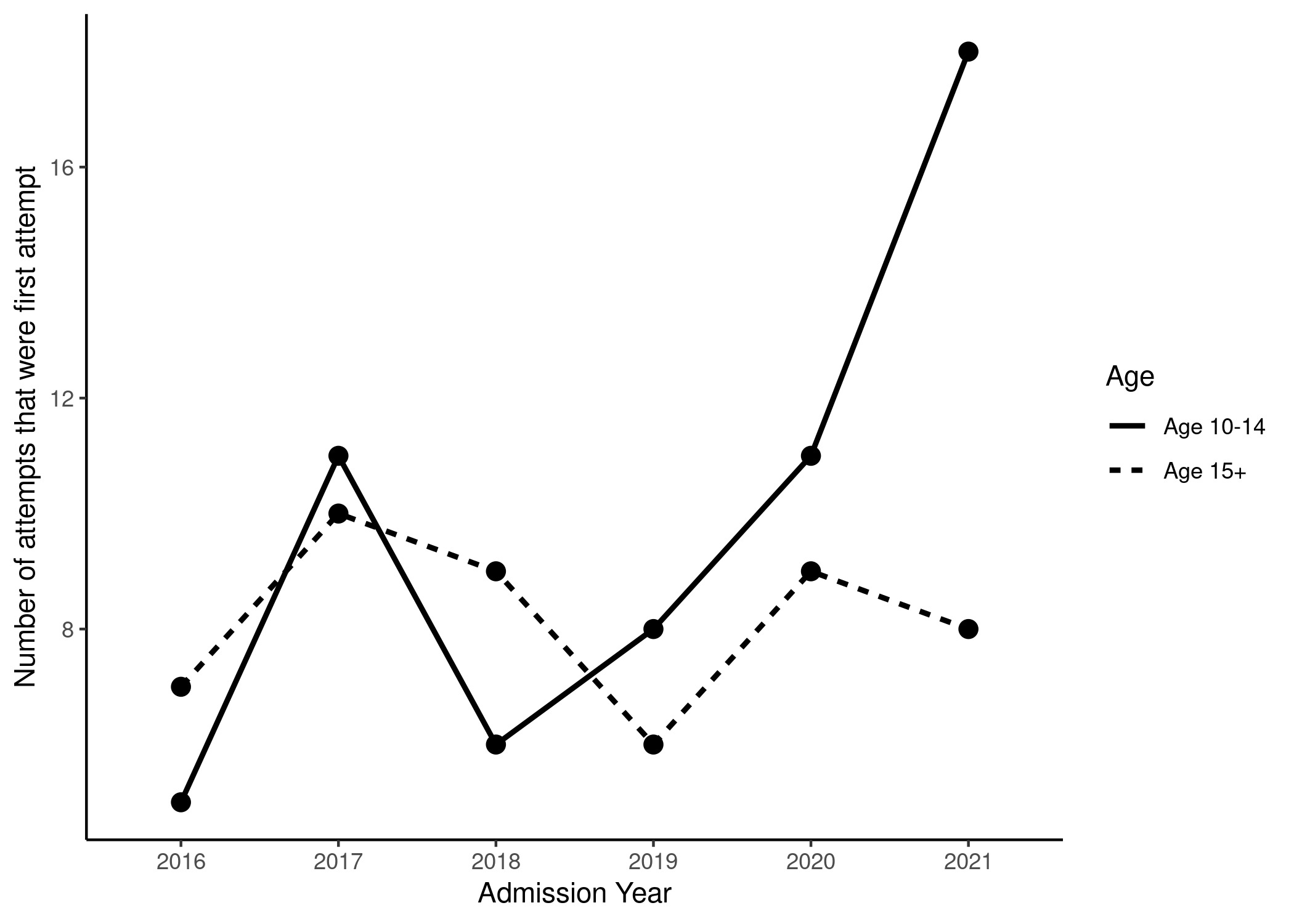
On average, age decreased 2.5 months with each year in the study period (Figure 1). The proportion of admitted patients who had never previously attempted suicide increased over time in the younger group (Figure 2). Rates of weekly or more marijuana use were significantly increased in the older age group (5.6% vs 27%, P = .003). Medication ingestion was the most common method of suicide attempt for all admissions (93%), with no difference between age groups (see Table 1, Clinical Characteristics).


Almost one-half of older adolescents (48%) and one-third of younger adolescents (32%) had a lifetime history of psychiatric admission for any reason. An almost identical trend existed for a previous, non-medically serious suicide attempt (47% and 32%, respectively). A psychosocial crisis within the preceding 24 hours was notably present in 43% of patients (see Table 1, Clinical History).
Discussion
This study demonstrates unique clinical and psychosocial patterns for youth who survive MSSAs, particularly regarding decreasing age, gender, and psychiatric history. Our data underscore the need for suicide prevention and intervention strategies that reflect these unique psychosocial factors. National data consistently demonstrate that female adolescents represent the majority of youth who attempt suicide, including those requiring medical attention.5 Females have been of particular concern among younger youth, specifically, with their suicide rate tripling, although males typically engage in more lethal methods and have a higher rate of suicide completion.6 Our study mirrored this pattern in younger female adolescents, with descriptive data identifying natal females as nearly three-quarters of admitted patients. However, this gap narrowed considerably in older teens to an almost even ratio, suggesting that males may be at elevated risk for more serious suicide attempts, in addition to completions.
We observed that the age of an index suicide attempt for youth in our study decreased over time (Figure 1), and the overall proportion of younger teens increased over time (Figure 2). We consider this to be a true increase and not directly confounded by other community variables, such as inpatient psychiatric bed availability or reduction in outpatient resources. Our hospital does not admit pediatric boarders waiting for psychiatric placement from the emergency department (ED); therefore, changes in bed availability would affect our length of stay but not our overall volume. Additionally, we would expect changes in community resources to affect both groups equally. Interestingly, noted proportional trends in younger youth did not follow annual overall volume changes of MSSA admissions.
Considerations driving this trend should include developmental immaturity and impulsivity inherent to younger adolescents, which may be a more pathological trait in older teens.7,8 Resulting ineffective coping strategies could easily combine with psychosocial stressors, even independent of contributing psychiatric illness. This could explain our data showing a psychosocial crisis within the previous 24 hours in 40% of all patients and in nearly one-half of older adolescents. This exceeds the one-third of suicidal decedents under age 18 previously determined through police and coroner/medical examiner data, per the National Vital Statistics System.9
Literature exists exploring the association between psychiatric hospitalization and future suicide risk. However, most studies focus primarily on the period immediately following or relatively soon after discharge and less on the medical seriousness of the preceding suicide attempt.10 Additionally, the relationship between pediatric MSSAs and the longitudinal risk of a preceding psychiatric hospitalization is underrepresented in the literature. Our study demonstrates unique findings including of a high rate of youth previously requiring an inpatient level of psychiatric care and a gap from psychiatric discharge being up to years prior.
The presence of preexisting psychiatric diagnoses has been demonstrated from psychological autopsies performed on completed youth suicides.2 Our data demonstrated a similar and expected pattern in an overwhelming majority of patients.7 Further research clarifying the specific diagnoses would help tailor suicide risk assessment approaches, as there are often already existing, but erroneous, assumptions regarding which diagnoses are the most relevant for effective suicide screening. Depression, for example, is often solely targeted, even though this approach has been demonstrated to miss up to one-third of youth at increased risk for suicide.11
Given the study period, it is also important to factor in potential influences of the COVID-19 pandemic. Literature from 2023 demonstrated strong evidence for relative increases in national ED visits for suicide attempts and ideation, and that the rate of suicide completion was higher than the expected rate during the first 10 months of the pandemic.12,13 However, it was also noted that these trends started prior to the pandemic, which then exacerbated, but did not create, the concerns. We believe this mimics the trends seen in our data, as we noted an overall rise in MSSAs prior to 2020. As a single-site study, we explored available data regarding deaths by suicide and ED presentations for suicidal ideation in Maine during the study period. It was clear that problematic trends in suicidal ideation and suicide completion for Maine youth also began well before the pandemic.13,14 For example, ED visits for adolescents aged 10–19 years evaluating suicidal ideation began rising after the first quarter of 2017 and continued to rise for almost every subsequent quarter through 2021, sometimes by as much as 40%.13,14 Similarly, suicide rates in children and teens began increasing before COVID-19 and, surprisingly, decreased between 2020 and 2021, which continued into 2023 before rising again post-pandemic.13,14 Unfortunately, data were not available for more specific age groups, so we are unable to comment on trends related only to younger or older adolescents. Another potential contributor to the noted MSSA increase in 2017 is the show “13 Reasons Why,” released in March of that year. An immediate increase in suicides beyond typical numbers occurred in 10- to 19-year-olds. Literature also documented temporal increases in youth self-harm, suicidal ideation, and suicide attempts.15 This could account for at least some of the overall volume increase in MSSAs seen at our institution in 2017.
Our study had several limitations. First, the sample size was small, and the lack of significant within-group effects may be due to inadequate statistical power. Second, as this was a single-site study, there may be limits to its generalizability. Finally, available data were limited to information provided by the patient and family when the full medical record was not within our health care system.
Conclusion
Youth admitted for MSSAs have been an underrepresented population in the literature. Our data support the claim that this population should continue to be explored separately to develop more effective suicide risk assessment, prevention, and monitoring strategies. Efforts should be made to raise awareness around heterogeneity in suicide risk profiles associated with diverse levels of potential lethality. This study provides a valuable perspective on this vulnerable population; however, future research would benefit from a prospective approach to better understand the impact of an MSSA on longitudinal suicide risk, which we are already undertaking as a separate study. Exploring youth who have repeated MSSAs would also be valuable, as they may represent their own unique cohort.
Plain Language Summary
Suicide remains a leading cause of death in youth, with ongoing and alarming trends at younger ages. Younger adolescents and preteens have become an alarming portion of patients admitted for serious suicide attempts, in addition to those dying by suicide. Refinement in screening and treatment is required.
About the Authors
Roslyn Gerwin, DO, Department of Psychiatry, Maine Medical Center, Portland, Maine, USA; Tufts University School of Medicine, Somerville, Massachusetts, USA.
Hannah Burley, MD, Department of Psychiatry, Maine Medical Center, Portland, Maine, USA; Tufts University School of Medicine, Somerville, Massachusetts, USA.
Anya Cutler, MS, MPH, MainHealth Institute for Research, Portland, Maine, USA.
Correspondence to: Roslyn Gerwin, DO; email: rlevine.gerwin@gmail.com, 207-662-5639, Maine Medical Center, 66 Bramhall Street, Portland, ME 04105.
Funding
Roslyn Gerwin, DO, had salary support from the Barbara Bush Children’s Hospital Scholarship Academy Faculty Resident Scholarship Program.
Disclosure
The authors have no conflicts of interest or financial relationships relevant to this article to disclose.
Acknowledgments
We wish to acknowledge the mentorship provided through the Barbara Bush Children’s Hospital Scholarship Academy and the MaineHealth Institute for Research, including Alexa Craig, MD and Leah Seften, BS.
Data Availability
Data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available as they contain information that could compromise the privacy of research participants.
Role of Funders
The funder did not participate in the work.
Ethical Considerations
This study was considered exempt according to the review policy of the medical center’s IRB. Protected Health Information with a correlation tool was stored in a separate, HIPAA-compliant database. Data analysis took place only on de-identified coded data.
Acknowledgement
This article is part of a special Clinical Perspectives series that will shed a new and focused light on clinically important topics within child and adolescent psychiatry. The series discusses the care of children and adolescents with psychiatric disorders from a new vantage point, including populations, practices, or clinical topics that may be otherwise overlooked. The series was edited by JAACAP Deputy Editor Lisa R. Fortuna, MD, MPH, MDiv, JAACAP Connect Editor David C. Saunders, MD, PhD, and JAACAP Editor-in-Chief Douglas K. Novins, MD.
Author Contributions
Conceptualization: Roslyn Gerwin (Lead), Hannah Burley (Supporting), Anya Cutler (Equal). Data curation: Roslyn Gerwin (Equal), Hannah Burley (Equal), Anya Cutler (Equal). Investigation: Roslyn Gerwin (Lead). Methodology: Roslyn Gerwin (Equal), Hannah Burley (Supporting), Anya Cutler (Equal). Supervision: Roslyn Gerwin (Lead). Writing – original draft: Roslyn Gerwin (Lead). Writing – review & editing: Roslyn Gerwin (Equal), Hannah Burley (Equal), Anya Cutler (Equal). Formal Analysis: Roslyn Gerwin (Equal), Hannah Burley (Equal), Anya Cutler (Lead). Funding acquisition: Roslyn Gerwin (Lead). Resources: Anya Cutler (Equal). Software: Anya Cutler (Lead). Validation: Anya Cutler (Lead).